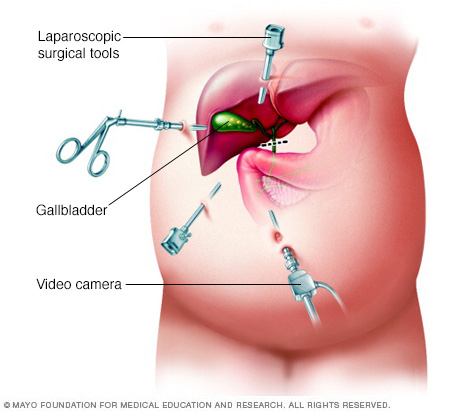
Laparoscopic cholecystectomy is a surgical procedure in which the doctor removes your gallbladder with the aid of a laparoscope. The gallbladder is a small pear-shaped organ on the underside of the liver that is used to store bile. A laparoscope is a small telescope, which is attached to a small camera and light source to enable the internal abdominal cavity to be visualized on a television screen. Three or four small (less than a cm each) incisions are made into the abdomen, through which the telescope and laparoscopic instruments are inserted. Gas is passed into the abdominal cavity to inflate it, so that the gallbladder can be seen more easily.
Laparoscopic (Keyhole) cholecystectomy is the most common way to remove the gallbladder today, but you should always keep in mind that cholecystectomy may not always be possible laparoscopically anda larger incision maybe needed to remove the gallbladder (open cholecystectomy technique).On the other hand, it is now also possible to perform cholecystectomy with a single small incision at the umbilicus (belly button). This new technique is known as SILS (single incision laparoscopic surgery). SILS cholecystectomy gives superior cosmetic results compared to even traditional laparoscopic cholecystectomy. You can ask us if you are a candidate for SILS cholecystectomy.
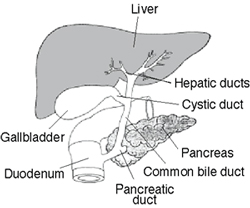
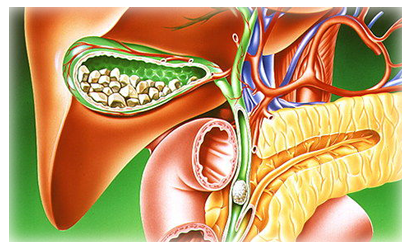
The liver produces a substance called bile. This is a green coloured liquid that helps the body to digest fats. Bile contains water, cholesterol, fats, bile salts and bilirubin. Bile salts break up the fat, and bilirubin gives stools their yellow-brown colour. The liver secretes bile into a branching network of small tubes called bile ducts, which join together to form a single large tube called common bile duct. The common bile duct opens into the duodenum, which is the initial part of the intestine just beyond the stomach. The gallbladder is connected to the common bile duct. Thus the bile flows from the liver to the common bile duct and into the gallbladder where it is temporarily stored when we are fasting. After we take a meal, the gallbladder contracts and empties bile into the duodenum where it helps to break down the fats.
Gallstones are formed when the bile stored in the gallbladder hardens into pieces of stone-like material. Gallstones are mainly composed of cholesterol. Most patients with gallstones remain symptom-free for many years and may, in fact, never develop any symptoms. Symptoms of gallstones are variable ranging from brief episodes of abdominal pain (known as biliary colic) to potentially life-threatening complications, such as acute inflammation and infection of the gallbladder (cholecystitis), inflammation of the pancreas (pancreatitis) and obstructive jaundice. It is accepted that the best treatment for gallstones that cause symptoms is the removal of the gallbladder by keyhole surgery (laparoscopic cholecystectomy). Occasionally surgery may be recommended for patients with gallstones in the absence of symptoms also.
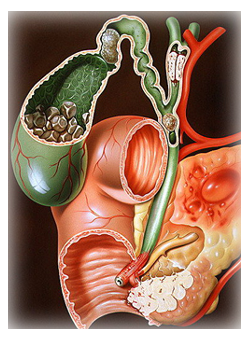
This procedure is performed when you have stones or inflammation in your gallbladder, causing pain. The gallbladder is shaped like a pear. It is attached to the undersurface of the liver. Bile produced in the liver is stored in the gallbladder. Concentrated and stagnant bile can form sediment in the gallbladder that can turn into gallstones. These stones may remain loose in your gallbladder or they may block the gallbladder outlet causing pain when the gallbladder contracts. In that case, the gallbladder may also become swollen, inflamed, and/or start (rarely) to decompose (become “gangrenous”). There are no alternatives to surgically removing the gallbladder when it is causing pain.
Gallstones that are confined to the gallbladder usually only cause intermittent episodes of pain, known as biliary colic. When a stone blocks the exit of the gallbladder the flow of bile is occluded, which can cause infection and inflammation of the gallbladder, called acute cholecystitis. A patient with acute cholecystitis may have a fever, severe upper right-sided abdominal pain and may vomit. When gallstones enter the common bile duct they can cause jaundice, cholangitis and pancreatitis. The stone blocking the flow of bile into the intestine causes jaundice. This leads to absorption of bilirubin into the bloodstream – causing yellow pigmentation of the skin and eyes. This absorbed bilirubin is excreted in the urine and gives it a dark yellow color. The obstruction of the common bile duct by a stone can also lead to infection in the biliary system. This is known as cholangitis. This infection can reach the liver if not treated promptly, and can result in inflammation of the liver and eventually liver abscesses. Pancreatitis occurs when a gallstone passing through the bile duct occludes the pancreatic duct leading to inflammation of the pancreas. The pancreatitis usually resolves if the gallstone passes out spontaneously into the duodenum. However, about 10 percent of patients with pancreatitis develop severe complications. Presence of gallstones in the common bile duct can be confirmed by doing an MRI of the abdomen known as MRCP (magnetic resonance cholangio-pancreatography) Common bile duct stones have to be removed in addition to removal of the gallbladder. These can be removed by an endoscopy performed by inserting a flexible tube through your month into your duodenum where the common bile duct opens followed by removal of gallstones in the common bile duct. This is known as endoscopic retrograde cholangio-pancreatography (ERCP).
ERCP is usually done prior to laparoscopic cholecystectomy. Occasionally it can be needed after the surgery if there is a stone detected in the common bile duct later. It is also possible to remove stones in the common bile duct surgicallyduring the laparoscopy procedure. This is known as laparoscopic common bile duct exploration. It is usually done for large stones in the common bile duct or when ERCP fails to remove stones Rare complications of gallstones include perforation of the gallbladder, erosion of the gallbladder into the bowel (cholecysto-enteral fistula) and passage of a gallstone into the bowel leading to a bowel obstruction. Occasionally due to certain difficulties encountered during laparoscopic cholecystectomy, the surgeon may prefer to convert to open cholecystectomy. The inflamed gallbladder is sometimes stuck to surrounding organs or there may be excessive bleeding during the surgery and therefore the surgeon may choose to perform an open cholecystectomy if he/she feels it is safer for the patient. Since this procedure is more invasive and leaves a larger scar, you will have a longer stay in hospital.
Having a laparoscopic cholecystectomy means that you will have a shorter recovery time, less pain, shorter hospital stay and will be able to return to work more quickly. With the laparoscopic cholecystectomy, you will probably have to stay in the hospital only for a day or two. On the other hand, an open cholecystectomy may increase your hospital stay to approximately 5 days. Also, because the incisions are much smaller with the laparoscopic technique you will find that the pain you experience will be a lot less than if you had the traditional open cholecystectomy.
The appendix produces a bacteria destroying protein called immunoglobulins, which help fight infection in the body. Its function, however, is not essential. People who have had appendectomies do not have an increased risk toward infection. Other organs in the body take over this function once the appendix has been removed.
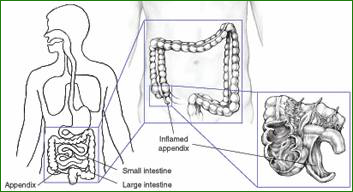
Appendicitis is a sudden inflammation of the appendix. Although the appendix does not seem to serve any purpose, it can become diseased and, of left untreated, can burst, causing infection and even death. The cause of appendicitis is usually unknown. Appendicitis may occur after a viral infection in the digestive tract or when the tube connecting the large intestine to the appendix is blocked or trapped by stool. It is thought that blockage of the opening of the appendix into the bowel by a hard, small stool fragment causes inflammation and infection of the appendix (appendicitis). This inflammation can cause infection, blood clot, or rupture of the appendix. The infected appendix then must be surgically removed (emergency appendectomy) before a hole develops in the appendix and the infection spreads to the abdominal space (peritonitis).
If you have any of these symptoms, see a doctor immediately. Appendicitis is considered to be an emergency because of the risk of rupture, which may happen as soon as 48 to 72 hours after symptoms begin.
The best treatment for appendicitis is to surgically remove the appendix. Mild appendicitis may sometimes be cured with antibiotics. More serious cases are treated with surgery, called an appendectomy or appendicectomy. Doctors either use an ‘open’ technique or a minimally invasive approach to remove the appendix.
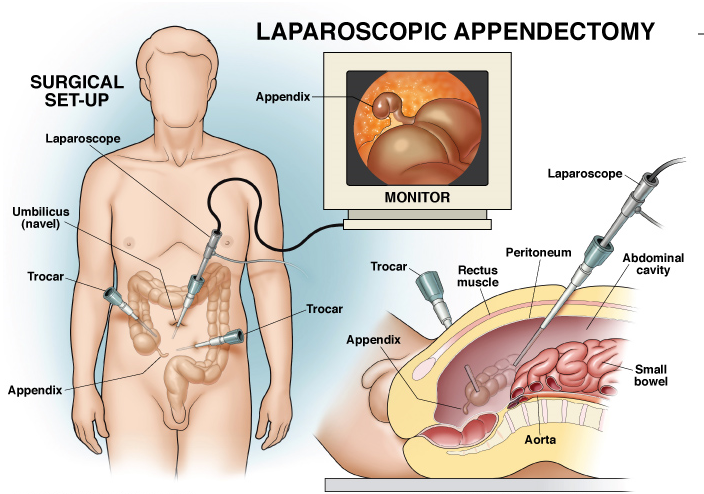
The laparoscopic (minimally invasive) technique involves making several tiny cuts in the abdomen and inserting a miniature camera and find laparoscopic instruments. The surgeon then removes the appendix with the instruments. This technique avoids the need to make a large incision in the abdomen and thus reduces post-operative pain and speeds up the recovery process.
In most cases, patients can be discharged within 24 – 36 hours after surgery. By contrast, the hospital stay is approximately 2 – 5 days for an open procedure.
Although “heartburn” is often used to describe a variety of digestive problems, in medical terms, it is actually a symptom of gastroesophageal reflux disease. In this condition, stomach acids reflux or “back up” from the stomach into the esophagus. Heartburn is described as a harsh, burning sensation in the area in between your ribs or just below your neck. The feeling may radiate through the chest and into the throat and neck. Many adults in the experience this uncomfortable burning sensation at least once a month. Other symptoms may also include vomiting, difficulty swallowing and chronic coughing or wheezing.
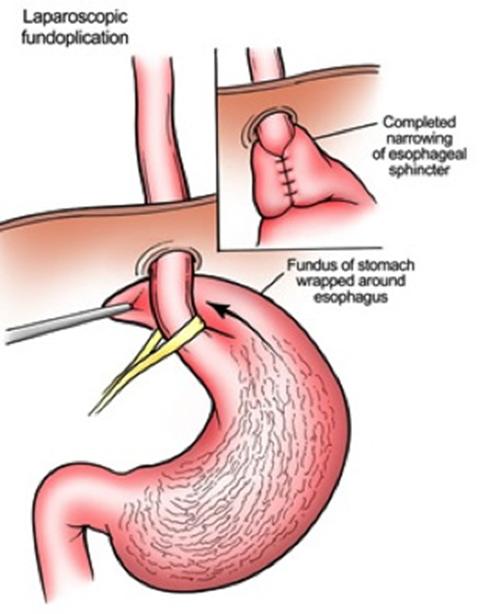
When you eat, food travels from your mouth to your stomach through a tube called the esophagus. At the lower end of the esophagus is a small ring of muscle called the lower esophageal sphincter (LES).
The LES acts like a one-way valve, allowing food to pass through into the stomach. Normally, the LES closes immediately after swallowing to prevent back-up of stomach juices, which have a high acid content, into the esophagus. GERD occurs when the LES does not function properly allowing acid to flow back and burn the lower esophagus. This irritates and inflames the esophagus, causing heartburn and eventually may damage the esophagus.
Some people are born with a naturally weak sphincter (LES). For others however, fatty and spicy foods, certain types of medication, tight clothing, smoking, drinking alcohol, vigorous exercise or changes in body position (bending over or lying down) may cause the LES to relax, causing reflux. A hiatal hernia (a common term for GERD) may be present in many patients who suffer from GERD, but may not cause symptoms of heartburn.
GERD is generally treated in three progressive steps:
In many cases, changing diet and taking over-the-counter antacids can reduce how often and how harsh your symptoms are. Losing weight, reducing or eliminating smoking and alcohol consumption, and altering eating and sleeping patterns can also help.
If symptoms persist after these life style changes, drug therapy may be required. Antacids neutralize stomach acids and over-the-counter medications reduce the amount of stomach acid produced. Both may be effective in relieving symptoms. Prescription drugs may be more effective in healing irritation of the esophagus and relieving symptoms. This therapy needs to be discussed with your surgeon.
Patients who do not respond well to lifestyle changes or medications or those who continually require medications to control their symptoms, will have to live with their condition or may undergo a surgical procedure. Surgery is very effective in treating GERD.There are procedures being tried, known as Intraluminal Endoscopic Procedures, which are alternatives to laparoscopic and open surgery. You will need to discuss with your surgeon and physician whether you are a candidate for any of these procedures.
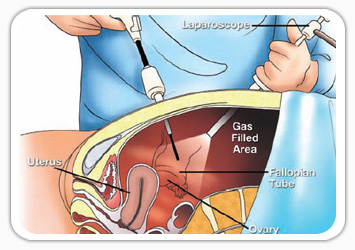
A laparoscope is a telescope designed for medical use. It is connected to a high intensity light and a high-resolution television camera so that the surgeon can see what is happening inside of you. The laparoscope is put into the abdominal cavity through a hollow tube and the image of the inside of your abdomen is seen on the television screen. In most cases, this procedure (operation) will be able to diagnose or help discover what the abdominal problem is.
Laparoscopy has a role in the diagnosis of both acute and chronic abdominal pain. There are many causes of abdominal pain. Some of these causes include appendicitis, adhesions or intra-abdominal scar tissue, pelvic infections, endometriosis, abdominal bleeding and, less frequently: cancer. It is used in patients with irritable bowel disease to exclude other causes of abdominal pain. Surgeons can often diagnose the cause of the abdominal pain and, during the same procedure, correct the problem.
A patient may have a lump (mass or tumour), which can be felt by the doctor, the patient, or seen on an X-ray. Most masses require a definitive diagnosis before appropriate therapy or treatment can be recommended. Laparoscopy is one of the techniques available to your physician to look directly at the mass and obtain tissue to discover the diagnosis.
The presence of fluid in the abdominal cavity is called ascites. Sometimes the cause of this fluid accumulation cannot be found without looking into the abdominal cavity, which can often be accomplished with laparoscopy.
Non-invasive X-ray imaging techniques (sonogram, CT scan and MRI) may discover a mass inside or on the surface of the liver. If the non-invasive X-ray cannot give your physician enough information, a liver biopsy may be needed to establish the diagnosis. Diagnostic laparoscopy is one of the safest and most accurate ways to obtain tissue for diagnosis. In other words, it is an accurate way to collect a biopsy to sample the liver or mass without actually opening the abdomen.
Your doctor may need information regarding the status of a previously treated disease, such as cancer. This may occur after treatment with some forms of chemotherapy or before more chemotherapy is started. Also, information may be provided by diagnostic laparoscopy before planning a formal exploration of the abdomen, chemotherapy or radiation therapy.
Ultrasound may be ordered by your doctor as a non-invasive diagnostic test. In many cases, information is provided which will allow your surgeon to have a better understanding of the problem inside your abdomen. This test is not painful, is very safe, and can improve the effectiveness of the diagnostic laparoscopy.
A CT Scan (X-ray)may be ordered which uses computers to visualize the intra-abdominal contents. In certain circumstances, it is accurate in making the diagnosis of abdominal disease. It will allow your surgeon to have a “road map” of the inside of your abdomen. A radiologist may use a CT scan to place a needle inside your abdomen. This is known as a CT guided needle biopsy. This will often be done before a diagnostic laparoscopy to decide if laparoscopy is appropriate for your condition.
An MRI (magnetic resonance imaging) may be ordered to view the inside of the abdominal cavity. It is not required for most abdominal problems, but may be necessary for some. Routine blood test analysis, urinalysis, and possible chest X-ray or electrocardiogram may be needed before diagnostic laparoscopy. Your physician will decide which tests are necessary and will review the results of those tests, which have already been performed.
For some patients, laparoscopic colon surgery is better tolerated in comparison to open surgery. While a small percent of patients undergoing laparoscopic colon surgery have to be changed to an open operation, the patients whose surgeries are completed by these minimally invasive techniques can enjoy a quicker recovery, less pain and a faster return to their normal life. The laparoscopic technique shares some of the same risks of any bowel operation, yet many studies show benefits of the laparoscopic technique.
If you or someone you know is faced with colon surgery and you want to consider the laparoscopic option, use our resources to find an experienced surgeon. If it is an emergency and you do not have ready access to an advanced laparoscopic surgeon, there is nothing wrong with open surgery. Do not hesitate, if you have the time, to ask your primary care physician or gastroenterologist to refer you to a qualified surgeon who will be glad to communicate with them about the plans and results of your treatment.
Some tests, such as a CAT scan(detailed Xray), may be ordered to see if there is any visible sign of the cancer having already spread. This could affect the decision for surgery as the finding of “metastasis” (spread) severely decreases (not to zero) the chance that the cancer can be cured. When surgery is done, the section of bowel with the tumour is removed along with some surrounding tissue. “Lymph nodes” will be checked for signs of cancer as this would be evidence that cancer cells had indeed already spread elsewhere. Other forms of “adjuvant” (additionally helpful) treatment may be recommended before or after the surgery.
Diverticulitis is a condition which may be caused by too many years of not enough fibre (roughage) in the diet and the colon squeezing so hard that pockets form. While most patients with diverticulosis (up to 50% of people by age 70) have no symptoms, each of these pockets can act like an appendix and can get infected, or even rupture.
The symptoms may range from vague, left lower abdominal pains with diarrhoea, constipation (or both); to severe pain, peritonitis or bowel blockage. In patients with mild symptoms, adding more fibre to the diet, with fruits, vegetables and whole grain cereals or with a supplement (such as fibre drinks), may help. It may also be necessary to undergo testing, such as a barium enema or colonoscopy, to exclude other possible conditions.
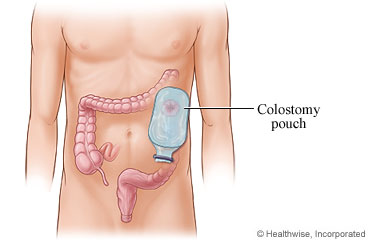
More severe symptoms usually respond to antibiotics, sometimes requiring administration through a vein in the hospital. People who get bad attacks again and again or have severe attacks, require surgery. Like colon cancer surgery, this surgery would require removal of the diseased section of the bowel possibly with construction of a colostomy.
Unless you are already hospitalized for a complication of your disease (such as bleeding or blockage), many colon surgery patients prepare their bowel for surgery while at home, coming to the hospital the day of surgery.
Traditionally, colon operations have been performed through large incisions running up and down the length of the abdomen. The section of the colon is removed, then the two ends of the bowel may be joined back together. The abdomen is closed and the patient is watched for any problems while waiting for their bowel to resume working so they can eat and go home. Normal activities with open operations may be restricted for a variable length of time.
Since the early 1990s, some surgeons, experienced both at colon surgery and laparoscopic surgery, have been removing the colon without a large incision, similar to the much more familiar gallbladder surgery.
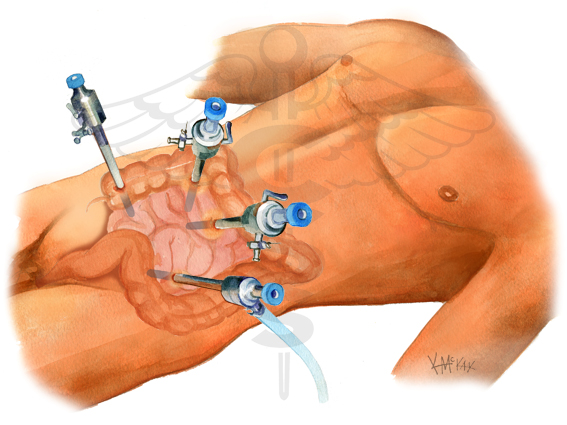
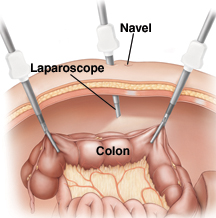
To do this surgery laparoscopically, the surgeon, instead of opening the skin large enough to work inside, places three to five “ports” in the patient, through which a video camera and miniature versions of the usual surgical instruments are passed. The surgical team then performs the same operation inside, without opening the abdomen to the air. The portion of bowel is removed by enlarging one of the port sites enough to pull the bowel portion out. Typically, there are then three or four incisions of 10mm or less and possibly one larger incision of several inches. Newer techniques include hand-assisted laparoscopic surgery.
There is typically less pain and a quicker return to normal intestinal and overall physical activity after the laparoscopic form of this operation.
Most patients faced with colon surgery are concerned over whether they will have to wear “a bag” (colostomy) into which their bowel empties. This is unusual in colon cancer cases unless the cancer is so low in the rectum that once removed, there is no bowel to hook back together. Colostomies are not unusual in emergency diverticulitis surgery as the bowel is so infected that joining it together immediately may not be safe. It may leak, requiring yet another operation. They are, however, usually temporary in this setting, and the patient can be brought back in for surgery to restore their usual bowel function in a few months. It is for this reason, however, that faced with repeated infections, a recommendation may be made for “elective” colon surgery as it can usually be completed in one stage.